In recent months, a large number of dangerous side effects of RNA- and virus-based (genetic) vaccinations have been observed. In contrast, immunization with the protein-based LubecaVax is almost free of side effects, and it results in high levels of neutralizing antibodies against corona viruses in 97% of vaccinated individuals. Due to its well-proven concept over many decades, this vaccination does not pose the innate risks which genetic vaccines reveal more and more.
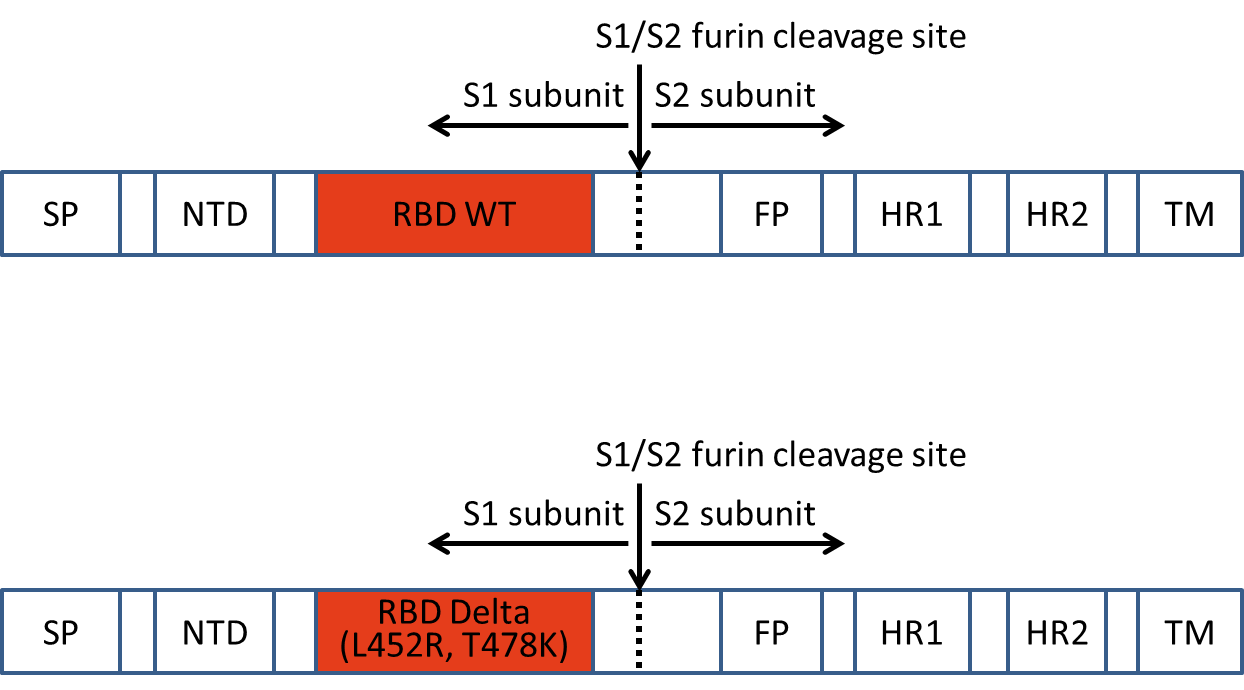
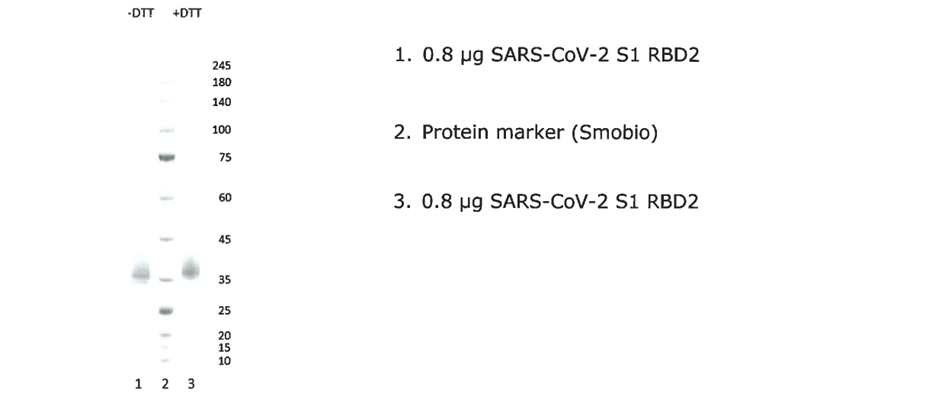
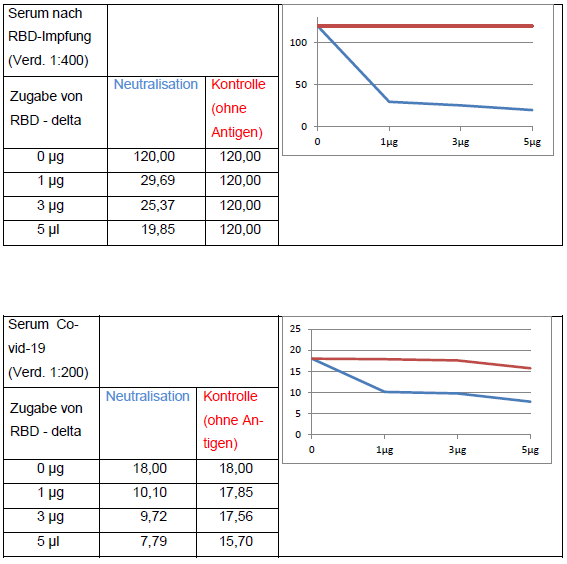
In the meantime, experience with the protein-based LubecaVax has been gained with about 60,000 vaccinations. They were started in March 2020, based on the receptor-binding domain (RBD) of the corona virus. Initially RBD of wild-type was used, since August 2021 RBD of the Delta virus, and since February 2022 RBD of Omicron plus wild-type. The vaccines do not contain any foreign genetic material – neither RNA nor the DNA of weakened viruses, and are by far better accepted by the public, since many people regard vaccinations with gene-ferries dangerous. LubecaVax hardly triggers allergic reactions, is low-priced and easy to be produced and to handle. Any physician can prepare it in his practice and administer it legally on an individual basis at the request of his patients. The components of the vaccine do not need to be transported deep-frozen and can be stored in the refrigerator (the few well-meant donations of provisionally approved vaccines in many cases fail due to logistics and the requirement of a cold chain).
The German Paul Ehrlich Institute either did not realize the potential of the Lübeck vaccine or eagerly wanted to leverage a new vaccination principle, which many scientists consider dangerous, and therefore blocked the way for an approval of the Lübeck vaccination. Having used the Lübeck anti-corona virus vaccine developed in March 2020 in the correct manner, the whole of Germany would presumably be free of the corona virus epidemic by now – if self-important authorities would not have prohibited the development and application of this vaccination.
In the warm season, in Germany the risk of infection with corona viruses is again very low. Also, the official vaccinations that have already been given (even though they are dangerous), may have contributed to herd immunity. But it is foreseeable that by the upcoming fall, the pandemic will have us firmly in its grip again. Vaccinated people should not be deceived into a false sense of security: Serum antibody levels for corona virus have been found to drop very rapidly, often to half or less within six months, so that people can soon become infected again after complete basic immunization (as we have experienced with the Delta-virus). However, even high levels do not protect against infection with more mutated variants (example Omicron), but the disease is usually very mild after immunization against wild type and Delta.
For the moment, it is therefore highly recommended to boost twice a year, in any case with an up-to-date recombinant antigen construct. A six-month break can be taken if the antibody concentration in the blood is sufficiently high, but this must be measured. Since RNA- and vector virus-based vaccinations can cause more and more damage with each further booster, only non-dangerous recombinant corona-RBD antigens should be used in the future, such as LubecaVax.
And here is my recommendation to the authorities in Germany: Let physicians exercise their right to treat their patients individually, if that is the patients’ intense desire. Stop depriving them of their basic constitutional right to produce and administer a vaccine in line with the freedom of choice of treatment. If the expectations come true that we will again have to immunize extensively against COVID-19 next fall, 10 million people will want to get a vaccine as LubecaVax. And they will not have to be forced by authorities to do so – what an opportunity! They are justly afraid of the state-ordered mass experiment with genetic vaccinations! They don’t want to be patronized and they don’t want a uniform press – we had that behind us long ago.
And another piece of advice to all the health authorities in our world: Don’t wait again several months before vaccinating when a new dangerous pathogen is spreading. As was shown with COVID-19, the genetic code of the virus and the epitopes suitable for vaccination were decoded within a few weeks of its first appearance. Let an institution have cell cultures on standby that can be used to produce harmless protein based vaccines (as in LubecaVax) in large quantities on short notice! The institution must already possess all approvals for such production.
Prof. Prof. h.c. (RCH) Dr. med. Winfried Stöcker
Further information can be found in the articles
“LubecaVax: The individual anti-corona vaccination from Lübeck”, version May 9, 2022 and
“Gene-based anti-corona vaccines are dangerous! The pseudo-COVID syndrome”, version May 3, 2022.